
IMEMR
EMRO
Volume 5, Issue 2 (2024)
J Clinic Care Skill 2024, 5(2): 85-91 |
Back to browse issues page
Article Type:
Subject:





History
Received: 2024/02/12 | Accepted: 2024/06/1 | Published: 2024/06/30
Received: 2024/02/12 | Accepted: 2024/06/1 | Published: 2024/06/30
How to cite this article
Sasani A, Rahzani K, Hekmatpou D, Haghverdi F. Comparing the Effect of Cryotherapy on Hugo Point and Needle Insertion Site on the Pain of Arteriovenous Fistula Cannulation in Patient with Hemodialysis. J Clinic Care Skill 2024; 5 (2) :85-91
URL: http://jccs.yums.ac.ir/article-1-242-en.html
URL: http://jccs.yums.ac.ir/article-1-242-en.html
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



Rights and permissions
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



1- Department of Nursing, Faculty of Nursing, Arak University of Medical Sciences, Arak, Iran
2- Department of Internal Medicine, Faculty of Medicine, Arak University of Medical Sciences, Arak, Iran
2- Department of Internal Medicine, Faculty of Medicine, Arak University of Medical Sciences, Arak, Iran
Full-Text (HTML) (1566 Views)
Introduction
Chronic kidney failure is a medical disorder characterized by the body's diminished capacity to regulate metabolic and electrolyte equilibrium, resulting in elevated levels of blood urea and nitrogen that are not properly eliminated from the body [1]. Hemodialysis is the predominant treatment modality for individuals with renal disease worldwide [2].
Hemodialysis is used to treat about 90% of individuals with chronic renal failure [3]. Hemodialysis is also the most widely used kidney replacement therapeutic technique in Iran. Every year, the number of patients receiving permanent hemodialysis rises by 15% [4, 5]. One of the physiological stresses experienced by these individuals is the pain that results from needle insertions into blood vessels both during and after hemodialysis [6]. Hemodialysis patients' lifeline is access to blood arteries, and the arteriovenous fistula (AVF) is the accepted and ideal technique [7, 8]. Hemodialysis requires the use of two venous and arterial needles [9]. One of the things that bothers these individuals during dialysis is the pain at the location where the needle enters the fistula. Several studies have indicated that 3.5% of hemodialysis patients experience severe fear due to needle insertion, while 22% report moderate fear [10]. Over 20% of these patients perceive the pain associated with vascular needle insertion as intolerable [11]. The repetitive nature of needle insertion for vascular access, coupled with the use of large dialysis needles, exacerbates this issue [12]. The stress and pain induced by needle insertion can lead to irritability, increased metabolism, catecholamine release, and alterations in vital signs such as elevated blood pressure and tachycardia, which are particularly detrimental to these patients given their advanced age and underlying health conditions [13]. Considering that hemodialysis typically occurs three times a week, with each session lasting 3 to 4 hours, patients endure needle-related stress and pain approximately 320 times annually. Consequently, effectively mitigating this pain and distress is a crucial aspect of patient care [14]. Ensuring patient comfort is vital for their long-term adaptation to treatment or until a successful kidney transplant is achieved [15].
In all pain-related guidelines, the patient's self-report is regarded as the most reliable tool for assessing pain and the most crucial element in pain evaluation. In Iran, currently, no specific measures are in place to reduce the pain associated with needle insertion during arteriovenous fistula (AVF) cannulation in hemodialysis patients. Only research studies have introduced pain reduction methods [16]. Skin stimulation is a standalone nursing intervention capable of alleviating patient pain [17]. Literature indicates that cryotherapy (cold therapy) is a form of skin stimulation that effectively reduces pain in hemodialysis patients during AVF needle insertion [15]. The pain reduction mechanism of cryotherapy is explained by the gate control theory of pain, as described by Ghani [18]. According to this theory, skin stimulation generates nerve impulses that are transmitted to the spinal cord and are either inhibited or amplified. Impulses traveling to the brain via smaller nerve fibers keep the pain gates open, while those traveling via larger fibers close the gate, thereby reducing pain perception. Stimulation of thick fibers through vibration or ice further enhances gate closure [19]. Cryotherapy decreases the temperature of the painful skin area, reducing nerve conduction in C and A-delta fibers and thus diminishing pain signal transmission [20]. Additionally, it reduces blood flow and cellular metabolism in the affected tissue [21], decreases inflammation [22], and ultimately promotes muscle relaxation and increases the pain threshold [23]. This method is straightforward, cost-effective, widely accessible, and devoid of side effects in pain reduction [24, 25].
Acupressure, a therapeutic method with a 5,000-year history, involves applying pressure to specific reflex points on the body's surface to reduce muscle tension and enhance blood flow and vital energy [24]. One of the most significant points, the Hugo point or LI-4, is located on the back of the hand between the thumb and index finger and is regarded as the primary anti-pain point in the body [26]. Stimulation of this acupoint can alleviate pain in various body regions. The Hugo point is situated where energy flow is close to the skin surface, making it easily accessible for stimulation through pressure, needles, or cold, thereby inhibiting the transmission of pain stimuli [27]. Moreover, stimulating this point activates the hypothalamus and pituitary glands, resulting in the release of endogenous opioids (endorphins) and subsequently reducing pain perception [28].
Studies have demonstrated the efficacy of cryotherapy at the Hugo point in reducing the pain associated with arteriovenous fistula (AVF) cannulation [29-31] and the impact of cryotherapy at the cannulation site of the fistula in decreasing pain intensity [15, 32]. In a study by Hosseinzadeh et al., the effects of cryotherapy at the Hugo point and acupressure at the Hugo point on AVF cannulation pain in hemodialysis patients were compared, with results indicating a greater effectiveness of cryotherapy [33].
Cryotherapy is recognized as a simple and cost-effective method; however, comprehensive research on the optimal site for cryotherapy has been lacking. Given the increasing number of patients requiring hemodialysis and the need to enhance nursing services, alongside the absence of research comparing cryotherapy at the Hugo point versus the AVF cannulation site for alleviating AVF cannulation pain, this study aimed to compare the effectiveness of these two cryotherapy methods on the pain intensity of AVF cannulation.
Materials and Methods
Study design
This study was conducted using a randomized clinical trial method in Arak City, Iran in 2023-2024.
Participants
The research community included patients undergoing hemodialysis at the Hami Hemodialysis Center in Arak. In this study, 56 hemodialysis patients participated. Two groups, cryotherapy at the Hugo point and cryotherapy at the arteriovenous fistula (AVF) cannulation site, were included in the study. This study was conducted from September 13 to November 21, 2023, at the Hami Hemodialysis Center in Arak.
The samples were selected through purposive sampling based on the inclusion criteria. The subjects were randomly assigned to two intervention groups, A (cryotherapy at the Hugo point) and B (cryotherapy at the fistula site) so that each group concluded 28 subjects by a systematic random sampling method. The sample size was determined by considering a type I error rate, the test power, mean (16.3) and standard deviation (17.2) of the first population, and the mean (54/1) and standard deviation (50.1) of the second population considering 10% potential decline rate,
The inclusion criteria were age range between 18-65 years, having normal consciousness and verbal and sensory abilities, non-emergency cannulation, and undergoing regular hemodialysis three times a week. The exclusion criteria included no allergy to cold, absence of numbness and neuropathy disorders at the cannulation site, no other pain except for cannulation pain in the hand, no history of psychiatric disorders, no use of narcotics or anesthetic drugs in the past 8 hours, and no skin problems such as eczema, burns, wounds, or cuts at the cannulation site.
Materials
Data were collected using assessing demographic information and the Visual Analog Scale (VAS). To collect demographic information, a researcher-developed checklist was used, comprising personal details (age, gender), socio-economic status (marital status, education level, occupation), medical history, and duration of dialysis.
The Visual Analog Scale (VAS) was used to determine pain intensity. This scale consists of a 10-centimeter line numbered from 0 (no pain) to 10 (worst possible pain). The visual scale for measuring pain intensity is a standard tool and is widely used in Iran. The validity and reliability of the pain measurement scale have been examined in numerous studies. Findings from Williamson and Hogarth's study regarding this tool indicate that it possesses adequate validity and reliability, making it practically useful in treatment settings [34].
The intervention was cryotherapy using an ice pack applied at the Hugo point and at the site of arteriovenous fistula cannulation.
In group A, cryotherapy involved placing an ice pack at the site of venous needle insertion. Prior to placing the ice pack, the entry point for the needle was marked. The ice pack was then applied for 10 minutes directly over the area where the venous needles enter, with moderate pressure applied clockwise (15 seconds of rest for every 2 minutes during the 10-minute period). After 10 minutes, the ice pack (YAKHPACK; Iran) was removed, the site was sterilized with alcohol swabs, and then cannulation was performed. Pain intensity was measured using the VAS tool within 1 minute after cannulation. The dimensions of the ice pack were approximately 10x10 cm and its weight was about 100 grams. According to the brochure, it is made of non-toxic gelatinous materials. The ice pack was frozen in a freezer for 2 hours, remained completely frozen, and maintained its temperature for up to 30 minutes.
Group B received cryotherapy at the Hugo point. In this method, the ice pack was applied for 10 minutes over the Hugo point, located between the index finger and thumb on the opposite side of the cannulation site on the back of the hand, with moderate pressure applied clockwise (15 seconds of rest for every 2 minutes during the 10 minutes). After 10 minutes, cannulation was performed, and pain intensity was measured using the VAS tool within 1 minute after cannulation.
All patients were standardized in terms of the type and thickness of the venous needle and the type of alcohol swab used. Venous cannulation for all patients was performed by a nurse from the dialysis unit.
The outcome measured was the pain resulting from venous cannulation in hemodialysis patients undergoing cryotherapy at the Hugo point and the site of arteriovenous fistula cannulation.
To avoid bias, the pain was assessed by individuals outside the study group. To prevent data leakage, sampling was conducted on alternating days (i.e., even and odd days), ensuring that patients had no contact or communication with each other.
Informed consent was obtained from the patients for participation in the study. The Helsinki Declaration guidelines were followed for the participants. Confidentiality and privacy were maintained. There was no financial cost or harm to the patients.
Data analysis
Data were analyzed using SPSS 23 software. The normality of the data was assessed using the Kolmogorov-Smirnov test. For qualitative variables, frequency and percentage were used, and for quantitative variables, mean and standard deviation indices were employed. Group comparisons regarding qualitative variables were conducted using the chi-square test, and for quantitative variables, an independent t-test or Mann-Whitney U test was used based on the normality of their distribution.
Findings
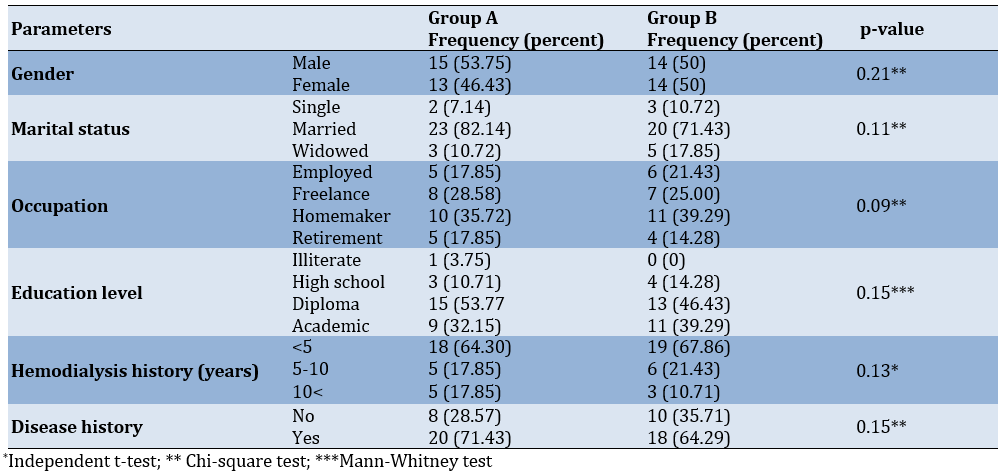
In both the Hugo point and catheterization site groups, the majority had less than 5 years of hemodialysis history, but the comparison of the frequency distribution of hemodialysis duration between the two groups did not show a significant difference (p>0.05). The majority in each group had underlying diseases, but a comparison of the frequency distribution of underlying disease status between the two acupuncture therapy groups did not show a significant difference (p>0.05; Table 1). The average age and standard deviation of the subjects were 64.60 (9.11) and 62.75 (8.85) for group A and B, respectively and there was no significant difference between two groups in terms of their ages (p-value=0.09; Table 1).
Table 1. Comparison of demographic and clinical information of participants
Although the mean intensity of pain from vascular needle insertion in the acupuncture therapy group at the needle insertion site was lower than the mean intensity of pain from vascular needle insertion in the acupuncture therapy group at the Hugo point, no statistically significant difference was observed between the two acupuncture therapy groups at the needle insertion site and Hugo point (p>0.05; Table 2).
Table 2. Comparison of mean pain intensity due to vascular needle insertion between subjects in group A and B within 1 minute after cannulation

Discussion
This study aimed to determine and compare the effect of cryotherapy at the Hugo point versus needle insertion site on pain caused by vascular needle insertion in hemodialysis patients. While previous studies have individually shown the effectiveness of cryotherapy at the Hugo point and needle insertion site compared to control groups, no study has directly compared these two methods. Therefore, this study is innovative in this regard.
The results showed no significant difference in the average pain intensity between the two cryotherapy groups at the site of vascular needle insertion and at the Hugo point. Comparing the average pain intensity caused by vascular needle insertion in the cryotherapy groups at the needle insertion site and Hugo point, within 1 minute after cannulation, indicated no significant difference in the average pain intensity of arteriovenous fistula cannulation. Although the average pain intensity was lower in the cryotherapy group at the needle insertion site, this difference was not statistically significant.
In contrast to our findings, Al Amer et al. [30] demonstrate that cryotherapy reduces pain related to arteriovenous fistula (AVF) cannulation. In their study, cryotherapy at the Huguenot site is compared with a control group, showing its effect, whereas the present study lacked a control group and compared the effects of cryotherapy at the Huguenot point and needle insertion site on AVF pain.
Kaviani et al. [31] compare the effects of two methods, pressure therapy, and ice massage at the Huguenot point, on pain intensity in primiparous women. The results indicate that the average pain score is lower in the pressure therapy and ice massage groups compared to the control group, but no significant difference in pain reduction is found between the two intervention groups [31]. In the present study, although cryotherapy at the Huguenot point was applied, which differs from the method used in the aforementioned study, similar to the previous study, no significant difference was observed between the effects of the two interventions.
Khosravan et al. [29] compare the effects of Hugo point massage (with and without ice) on pain caused by pentavalent vaccine injection. Their results show that both methods of massage, with and without ice, are effective in reducing vaccination pain in infants and have a significant difference compared with the control group. However, there is no significant difference between the two intervention methods, although ice massage is more effective than massage without ice. In the present study, although the average pain in the group with cryotherapy at the Hegu point was higher than with cryotherapy for arteriovenous fistula cannulation, similar to the aforementioned study, no significant difference was found between the effects of the two methods on patient pain.
Additionally, Soltanpour [35] indicate that ice massage at the Hugo point is an effective method for relieving pain caused by needle insertion into an arteriovenous fistula [36]. Although there was no control group in this study, the effect of cryotherapy at the Hugo point on pain was not compared with a control group, but the pain level was moderate.
Arabet al. [20] compare the effects of Hugo point ice massage and 2% lidocaine gel on pain caused by needle insertion into an arteriovenous fistula in hemodialysis patients. The results demonstrate that both interventions effectively reduce pain, but the effect of cryotherapy at the Hugo point is significantly greater than that of lidocaine [20]. In the above study, the pain before the interventions is also assessed in the first session, and the interventions are applied in the subsequent session. Therefore, the effects of each intervention are compared, and the cryotherapy intervention is performed for a longer duration. However, in the present study, the pain of needle insertion into the arteriovenous fistula was not measured without the intervention.
In the study by Golda et al., the results show that the average pain intensity after the test in hemodialysis patients is 1.53 in the ice massage intervention group and 5.7 in the control group. The difference in average pain intensity during venipuncture between the two groups is statistically significant [32]. In the present study, the average pain in both groups was lower than the control group in the above study; although the pain intensity in both intervention groups was higher than in the above study. This difference may indicate that cryotherapy at both the arteriovenous fistula site and the Hugo point reduced pain in the present study. However, the higher pain in the intervention groups in this study is likely due to the different times of pain measurement. Moreover, considering the subjective nature of pain, precise pain measurement is not possible.
Given the negative effects of pain caused by the puncturing of arteriovenous fistulas on the physical and mental health of hemodialysis patients, pain control in these patients is very important. Pourramzani et al. report that cryotherapy at the Hugo point reduces the pain intensity of arteriovenous fistula cannulation and can be suggested as an effective non-invasive method for relieving pain caused by puncturing in hemodialysis patients [36]. According to the results of a review article, cryotherapy has a positive effect on reducing pain caused by puncturing arteriovenous fistulas in hemodialysis patients [15]. Therefore, considering the positive effect of cryotherapy in reducing pain caused by fistula puncturing, cryotherapy seems to be an effective and useful low-risk and complication-free method for reducing pain and ultimately reducing the unpleasant psychological and physical effects of pain. According to patients' rights and Maslow's hierarchy of needs, pain relief is one of the basic human needs [37]. Both pharmacological and non-pharmacological methods are used for pain relief. However, non-pharmacological methods are preferred. Studies have shown that skin stimulation is an independent nursing intervention that leads to pain relief [38]. Cryotherapy is an effective method of skin stimulation. It is cost-effective, has few complications, is easy to use, and does not have side effects like skin rash, erythema, and itching caused by topical anesthetics such as EMLA cream, lidocaine, and other drugs [39].
In the present study, although cryotherapy intervention at the needle entry site of the arteriovenous fistula resulted in less pain compared to cryotherapy at the Hugo point, the difference was not significant. Therefore, considering that in the above studies, cryotherapy at the Hugo point and the arteriovenous fistula cannulation site have both resulted in pain reduction during arteriovenous fistula cannulation, either method-cryotherapy at the Hugo point or especially cryotherapy at the arteriovenous fistula cannulation site can be suggested as an independent nursing intervention and a non-invasive, complication-free pain relief method to reduce pain during arteriovenous fistula cannulation in hospitalized patients, particularly those undergoing hemodialysis. These results can be utilized by nurses and other healthcare personnel for pain management in patients requiring injections.
Suggestions and limitations
One of the limitations of this study is the lack of a control group. However, considering that previous studies show each of these two interventions reduce pain in the intervention group compared to the control group [20, 29, 30, 32, 35], the methodologists deemed a control group unnecessary for comparison purposes. Therefore, this study was conducted solely to compare the two cryotherapy methods at the Hugo point and the needle entry site of the arteriovenous fistula. Another limitation was the absence of pain measurement at the needle entry site in these participants during sessions prior to the intervention. Additionally, the subjective nature of pain measurement using the VRS scale, especially when measuring pain 1 minute after injection, may not provide an accurate assessment of pain.
Further studies with larger sample sizes, including control groups and pain measurement at the needle entry site during a session prior to the intervention session, as well as the application of the intervention multiple times and over a longer duration for each individual, are necessary to investigate and compare the impact of these two interventions on pain reduction in hemodialysis patients.
Cryotherapy at both the Hugo point and the needle entry site of the arteriovenous fistula can reduce the pain intensity associated with venipuncture in hemodialysis patients, and both methods can be recommended for reducing needle entry site pain.
Conclusion
Cryotherapy intervention at the needle insertion site and Hugo's point has the same effect on reducing arteriovenous fistula cannulation pain.
Acknowledgments: This research is derived from the master's thesis of Ms. Atefeh Sasani, which was approved at Arak University of Medical Sciences. We hereby express our gratitude to the university's research department, as well as all the officials, staff, and patients attending the Hami Arak Hemodialysis Center.
Ethical Permission: This research received ethical approval from the Ethics Committee of Arak University of Medical Sciences with the identifier IR.ARAKMU.REC.1400.329. This study is registered on the Iranian Registry of Clinical Trials with the number IRCT20220612055152N1.
Conflict of Interest: There are no conflicts of interest. This study was financially supported by the Research Department of Arak University of Medical Sciences.
Authors’ Contribution: Sasani A (First Author), Main Researcher/Introduction Writer/Methodologist/ Discussion Writer/Statistical Analyst (30%); Rahzani K (Second Author), Main Researcher/Introduction Writer/Methodologist/Discussion Writer/Statistical Analyst (30%); Hekmatpour D (Third Author), Assistant Researcher/Introduction Writer/Discussion Writer (20%); Haghverdi F (Forth Author), Assistant Researcher/ Statistical Analyst/ Discussion Writer (20%).
Funding/Support: This study was financially supported by the Research Department of Arak University of Medical Sciences.
Chronic kidney failure is a medical disorder characterized by the body's diminished capacity to regulate metabolic and electrolyte equilibrium, resulting in elevated levels of blood urea and nitrogen that are not properly eliminated from the body [1]. Hemodialysis is the predominant treatment modality for individuals with renal disease worldwide [2].
Hemodialysis is used to treat about 90% of individuals with chronic renal failure [3]. Hemodialysis is also the most widely used kidney replacement therapeutic technique in Iran. Every year, the number of patients receiving permanent hemodialysis rises by 15% [4, 5]. One of the physiological stresses experienced by these individuals is the pain that results from needle insertions into blood vessels both during and after hemodialysis [6]. Hemodialysis patients' lifeline is access to blood arteries, and the arteriovenous fistula (AVF) is the accepted and ideal technique [7, 8]. Hemodialysis requires the use of two venous and arterial needles [9]. One of the things that bothers these individuals during dialysis is the pain at the location where the needle enters the fistula. Several studies have indicated that 3.5% of hemodialysis patients experience severe fear due to needle insertion, while 22% report moderate fear [10]. Over 20% of these patients perceive the pain associated with vascular needle insertion as intolerable [11]. The repetitive nature of needle insertion for vascular access, coupled with the use of large dialysis needles, exacerbates this issue [12]. The stress and pain induced by needle insertion can lead to irritability, increased metabolism, catecholamine release, and alterations in vital signs such as elevated blood pressure and tachycardia, which are particularly detrimental to these patients given their advanced age and underlying health conditions [13]. Considering that hemodialysis typically occurs three times a week, with each session lasting 3 to 4 hours, patients endure needle-related stress and pain approximately 320 times annually. Consequently, effectively mitigating this pain and distress is a crucial aspect of patient care [14]. Ensuring patient comfort is vital for their long-term adaptation to treatment or until a successful kidney transplant is achieved [15].
In all pain-related guidelines, the patient's self-report is regarded as the most reliable tool for assessing pain and the most crucial element in pain evaluation. In Iran, currently, no specific measures are in place to reduce the pain associated with needle insertion during arteriovenous fistula (AVF) cannulation in hemodialysis patients. Only research studies have introduced pain reduction methods [16]. Skin stimulation is a standalone nursing intervention capable of alleviating patient pain [17]. Literature indicates that cryotherapy (cold therapy) is a form of skin stimulation that effectively reduces pain in hemodialysis patients during AVF needle insertion [15]. The pain reduction mechanism of cryotherapy is explained by the gate control theory of pain, as described by Ghani [18]. According to this theory, skin stimulation generates nerve impulses that are transmitted to the spinal cord and are either inhibited or amplified. Impulses traveling to the brain via smaller nerve fibers keep the pain gates open, while those traveling via larger fibers close the gate, thereby reducing pain perception. Stimulation of thick fibers through vibration or ice further enhances gate closure [19]. Cryotherapy decreases the temperature of the painful skin area, reducing nerve conduction in C and A-delta fibers and thus diminishing pain signal transmission [20]. Additionally, it reduces blood flow and cellular metabolism in the affected tissue [21], decreases inflammation [22], and ultimately promotes muscle relaxation and increases the pain threshold [23]. This method is straightforward, cost-effective, widely accessible, and devoid of side effects in pain reduction [24, 25].
Acupressure, a therapeutic method with a 5,000-year history, involves applying pressure to specific reflex points on the body's surface to reduce muscle tension and enhance blood flow and vital energy [24]. One of the most significant points, the Hugo point or LI-4, is located on the back of the hand between the thumb and index finger and is regarded as the primary anti-pain point in the body [26]. Stimulation of this acupoint can alleviate pain in various body regions. The Hugo point is situated where energy flow is close to the skin surface, making it easily accessible for stimulation through pressure, needles, or cold, thereby inhibiting the transmission of pain stimuli [27]. Moreover, stimulating this point activates the hypothalamus and pituitary glands, resulting in the release of endogenous opioids (endorphins) and subsequently reducing pain perception [28].
Studies have demonstrated the efficacy of cryotherapy at the Hugo point in reducing the pain associated with arteriovenous fistula (AVF) cannulation [29-31] and the impact of cryotherapy at the cannulation site of the fistula in decreasing pain intensity [15, 32]. In a study by Hosseinzadeh et al., the effects of cryotherapy at the Hugo point and acupressure at the Hugo point on AVF cannulation pain in hemodialysis patients were compared, with results indicating a greater effectiveness of cryotherapy [33].
Cryotherapy is recognized as a simple and cost-effective method; however, comprehensive research on the optimal site for cryotherapy has been lacking. Given the increasing number of patients requiring hemodialysis and the need to enhance nursing services, alongside the absence of research comparing cryotherapy at the Hugo point versus the AVF cannulation site for alleviating AVF cannulation pain, this study aimed to compare the effectiveness of these two cryotherapy methods on the pain intensity of AVF cannulation.
Materials and Methods
Study design
This study was conducted using a randomized clinical trial method in Arak City, Iran in 2023-2024.
Participants
The research community included patients undergoing hemodialysis at the Hami Hemodialysis Center in Arak. In this study, 56 hemodialysis patients participated. Two groups, cryotherapy at the Hugo point and cryotherapy at the arteriovenous fistula (AVF) cannulation site, were included in the study. This study was conducted from September 13 to November 21, 2023, at the Hami Hemodialysis Center in Arak.
The samples were selected through purposive sampling based on the inclusion criteria. The subjects were randomly assigned to two intervention groups, A (cryotherapy at the Hugo point) and B (cryotherapy at the fistula site) so that each group concluded 28 subjects by a systematic random sampling method. The sample size was determined by considering a type I error rate, the test power, mean (16.3) and standard deviation (17.2) of the first population, and the mean (54/1) and standard deviation (50.1) of the second population considering 10% potential decline rate,
The inclusion criteria were age range between 18-65 years, having normal consciousness and verbal and sensory abilities, non-emergency cannulation, and undergoing regular hemodialysis three times a week. The exclusion criteria included no allergy to cold, absence of numbness and neuropathy disorders at the cannulation site, no other pain except for cannulation pain in the hand, no history of psychiatric disorders, no use of narcotics or anesthetic drugs in the past 8 hours, and no skin problems such as eczema, burns, wounds, or cuts at the cannulation site.
Materials
Data were collected using assessing demographic information and the Visual Analog Scale (VAS). To collect demographic information, a researcher-developed checklist was used, comprising personal details (age, gender), socio-economic status (marital status, education level, occupation), medical history, and duration of dialysis.
The Visual Analog Scale (VAS) was used to determine pain intensity. This scale consists of a 10-centimeter line numbered from 0 (no pain) to 10 (worst possible pain). The visual scale for measuring pain intensity is a standard tool and is widely used in Iran. The validity and reliability of the pain measurement scale have been examined in numerous studies. Findings from Williamson and Hogarth's study regarding this tool indicate that it possesses adequate validity and reliability, making it practically useful in treatment settings [34].
The intervention was cryotherapy using an ice pack applied at the Hugo point and at the site of arteriovenous fistula cannulation.
In group A, cryotherapy involved placing an ice pack at the site of venous needle insertion. Prior to placing the ice pack, the entry point for the needle was marked. The ice pack was then applied for 10 minutes directly over the area where the venous needles enter, with moderate pressure applied clockwise (15 seconds of rest for every 2 minutes during the 10-minute period). After 10 minutes, the ice pack (YAKHPACK; Iran) was removed, the site was sterilized with alcohol swabs, and then cannulation was performed. Pain intensity was measured using the VAS tool within 1 minute after cannulation. The dimensions of the ice pack were approximately 10x10 cm and its weight was about 100 grams. According to the brochure, it is made of non-toxic gelatinous materials. The ice pack was frozen in a freezer for 2 hours, remained completely frozen, and maintained its temperature for up to 30 minutes.
Group B received cryotherapy at the Hugo point. In this method, the ice pack was applied for 10 minutes over the Hugo point, located between the index finger and thumb on the opposite side of the cannulation site on the back of the hand, with moderate pressure applied clockwise (15 seconds of rest for every 2 minutes during the 10 minutes). After 10 minutes, cannulation was performed, and pain intensity was measured using the VAS tool within 1 minute after cannulation.
All patients were standardized in terms of the type and thickness of the venous needle and the type of alcohol swab used. Venous cannulation for all patients was performed by a nurse from the dialysis unit.
The outcome measured was the pain resulting from venous cannulation in hemodialysis patients undergoing cryotherapy at the Hugo point and the site of arteriovenous fistula cannulation.
To avoid bias, the pain was assessed by individuals outside the study group. To prevent data leakage, sampling was conducted on alternating days (i.e., even and odd days), ensuring that patients had no contact or communication with each other.
Informed consent was obtained from the patients for participation in the study. The Helsinki Declaration guidelines were followed for the participants. Confidentiality and privacy were maintained. There was no financial cost or harm to the patients.
Data analysis
Data were analyzed using SPSS 23 software. The normality of the data was assessed using the Kolmogorov-Smirnov test. For qualitative variables, frequency and percentage were used, and for quantitative variables, mean and standard deviation indices were employed. Group comparisons regarding qualitative variables were conducted using the chi-square test, and for quantitative variables, an independent t-test or Mann-Whitney U test was used based on the normality of their distribution.
Findings
In both the Hugo point and catheterization site groups, the majority had less than 5 years of hemodialysis history, but the comparison of the frequency distribution of hemodialysis duration between the two groups did not show a significant difference (p>0.05). The majority in each group had underlying diseases, but a comparison of the frequency distribution of underlying disease status between the two acupuncture therapy groups did not show a significant difference (p>0.05; Table 1). The average age and standard deviation of the subjects were 64.60 (9.11) and 62.75 (8.85) for group A and B, respectively and there was no significant difference between two groups in terms of their ages (p-value=0.09; Table 1).
Table 1. Comparison of demographic and clinical information of participants
Although the mean intensity of pain from vascular needle insertion in the acupuncture therapy group at the needle insertion site was lower than the mean intensity of pain from vascular needle insertion in the acupuncture therapy group at the Hugo point, no statistically significant difference was observed between the two acupuncture therapy groups at the needle insertion site and Hugo point (p>0.05; Table 2).
Table 2. Comparison of mean pain intensity due to vascular needle insertion between subjects in group A and B within 1 minute after cannulation
Discussion
This study aimed to determine and compare the effect of cryotherapy at the Hugo point versus needle insertion site on pain caused by vascular needle insertion in hemodialysis patients. While previous studies have individually shown the effectiveness of cryotherapy at the Hugo point and needle insertion site compared to control groups, no study has directly compared these two methods. Therefore, this study is innovative in this regard.
The results showed no significant difference in the average pain intensity between the two cryotherapy groups at the site of vascular needle insertion and at the Hugo point. Comparing the average pain intensity caused by vascular needle insertion in the cryotherapy groups at the needle insertion site and Hugo point, within 1 minute after cannulation, indicated no significant difference in the average pain intensity of arteriovenous fistula cannulation. Although the average pain intensity was lower in the cryotherapy group at the needle insertion site, this difference was not statistically significant.
In contrast to our findings, Al Amer et al. [30] demonstrate that cryotherapy reduces pain related to arteriovenous fistula (AVF) cannulation. In their study, cryotherapy at the Huguenot site is compared with a control group, showing its effect, whereas the present study lacked a control group and compared the effects of cryotherapy at the Huguenot point and needle insertion site on AVF pain.
Kaviani et al. [31] compare the effects of two methods, pressure therapy, and ice massage at the Huguenot point, on pain intensity in primiparous women. The results indicate that the average pain score is lower in the pressure therapy and ice massage groups compared to the control group, but no significant difference in pain reduction is found between the two intervention groups [31]. In the present study, although cryotherapy at the Huguenot point was applied, which differs from the method used in the aforementioned study, similar to the previous study, no significant difference was observed between the effects of the two interventions.
Khosravan et al. [29] compare the effects of Hugo point massage (with and without ice) on pain caused by pentavalent vaccine injection. Their results show that both methods of massage, with and without ice, are effective in reducing vaccination pain in infants and have a significant difference compared with the control group. However, there is no significant difference between the two intervention methods, although ice massage is more effective than massage without ice. In the present study, although the average pain in the group with cryotherapy at the Hegu point was higher than with cryotherapy for arteriovenous fistula cannulation, similar to the aforementioned study, no significant difference was found between the effects of the two methods on patient pain.
Additionally, Soltanpour [35] indicate that ice massage at the Hugo point is an effective method for relieving pain caused by needle insertion into an arteriovenous fistula [36]. Although there was no control group in this study, the effect of cryotherapy at the Hugo point on pain was not compared with a control group, but the pain level was moderate.
Arabet al. [20] compare the effects of Hugo point ice massage and 2% lidocaine gel on pain caused by needle insertion into an arteriovenous fistula in hemodialysis patients. The results demonstrate that both interventions effectively reduce pain, but the effect of cryotherapy at the Hugo point is significantly greater than that of lidocaine [20]. In the above study, the pain before the interventions is also assessed in the first session, and the interventions are applied in the subsequent session. Therefore, the effects of each intervention are compared, and the cryotherapy intervention is performed for a longer duration. However, in the present study, the pain of needle insertion into the arteriovenous fistula was not measured without the intervention.
In the study by Golda et al., the results show that the average pain intensity after the test in hemodialysis patients is 1.53 in the ice massage intervention group and 5.7 in the control group. The difference in average pain intensity during venipuncture between the two groups is statistically significant [32]. In the present study, the average pain in both groups was lower than the control group in the above study; although the pain intensity in both intervention groups was higher than in the above study. This difference may indicate that cryotherapy at both the arteriovenous fistula site and the Hugo point reduced pain in the present study. However, the higher pain in the intervention groups in this study is likely due to the different times of pain measurement. Moreover, considering the subjective nature of pain, precise pain measurement is not possible.
Given the negative effects of pain caused by the puncturing of arteriovenous fistulas on the physical and mental health of hemodialysis patients, pain control in these patients is very important. Pourramzani et al. report that cryotherapy at the Hugo point reduces the pain intensity of arteriovenous fistula cannulation and can be suggested as an effective non-invasive method for relieving pain caused by puncturing in hemodialysis patients [36]. According to the results of a review article, cryotherapy has a positive effect on reducing pain caused by puncturing arteriovenous fistulas in hemodialysis patients [15]. Therefore, considering the positive effect of cryotherapy in reducing pain caused by fistula puncturing, cryotherapy seems to be an effective and useful low-risk and complication-free method for reducing pain and ultimately reducing the unpleasant psychological and physical effects of pain. According to patients' rights and Maslow's hierarchy of needs, pain relief is one of the basic human needs [37]. Both pharmacological and non-pharmacological methods are used for pain relief. However, non-pharmacological methods are preferred. Studies have shown that skin stimulation is an independent nursing intervention that leads to pain relief [38]. Cryotherapy is an effective method of skin stimulation. It is cost-effective, has few complications, is easy to use, and does not have side effects like skin rash, erythema, and itching caused by topical anesthetics such as EMLA cream, lidocaine, and other drugs [39].
In the present study, although cryotherapy intervention at the needle entry site of the arteriovenous fistula resulted in less pain compared to cryotherapy at the Hugo point, the difference was not significant. Therefore, considering that in the above studies, cryotherapy at the Hugo point and the arteriovenous fistula cannulation site have both resulted in pain reduction during arteriovenous fistula cannulation, either method-cryotherapy at the Hugo point or especially cryotherapy at the arteriovenous fistula cannulation site can be suggested as an independent nursing intervention and a non-invasive, complication-free pain relief method to reduce pain during arteriovenous fistula cannulation in hospitalized patients, particularly those undergoing hemodialysis. These results can be utilized by nurses and other healthcare personnel for pain management in patients requiring injections.
Suggestions and limitations
One of the limitations of this study is the lack of a control group. However, considering that previous studies show each of these two interventions reduce pain in the intervention group compared to the control group [20, 29, 30, 32, 35], the methodologists deemed a control group unnecessary for comparison purposes. Therefore, this study was conducted solely to compare the two cryotherapy methods at the Hugo point and the needle entry site of the arteriovenous fistula. Another limitation was the absence of pain measurement at the needle entry site in these participants during sessions prior to the intervention. Additionally, the subjective nature of pain measurement using the VRS scale, especially when measuring pain 1 minute after injection, may not provide an accurate assessment of pain.
Further studies with larger sample sizes, including control groups and pain measurement at the needle entry site during a session prior to the intervention session, as well as the application of the intervention multiple times and over a longer duration for each individual, are necessary to investigate and compare the impact of these two interventions on pain reduction in hemodialysis patients.
Cryotherapy at both the Hugo point and the needle entry site of the arteriovenous fistula can reduce the pain intensity associated with venipuncture in hemodialysis patients, and both methods can be recommended for reducing needle entry site pain.
Conclusion
Cryotherapy intervention at the needle insertion site and Hugo's point has the same effect on reducing arteriovenous fistula cannulation pain.
Acknowledgments: This research is derived from the master's thesis of Ms. Atefeh Sasani, which was approved at Arak University of Medical Sciences. We hereby express our gratitude to the university's research department, as well as all the officials, staff, and patients attending the Hami Arak Hemodialysis Center.
Ethical Permission: This research received ethical approval from the Ethics Committee of Arak University of Medical Sciences with the identifier IR.ARAKMU.REC.1400.329. This study is registered on the Iranian Registry of Clinical Trials with the number IRCT20220612055152N1.
Conflict of Interest: There are no conflicts of interest. This study was financially supported by the Research Department of Arak University of Medical Sciences.
Authors’ Contribution: Sasani A (First Author), Main Researcher/Introduction Writer/Methodologist/ Discussion Writer/Statistical Analyst (30%); Rahzani K (Second Author), Main Researcher/Introduction Writer/Methodologist/Discussion Writer/Statistical Analyst (30%); Hekmatpour D (Third Author), Assistant Researcher/Introduction Writer/Discussion Writer (20%); Haghverdi F (Forth Author), Assistant Researcher/ Statistical Analyst/ Discussion Writer (20%).
Funding/Support: This study was financially supported by the Research Department of Arak University of Medical Sciences.
Keywords:
References
1. Moradi M, Parker M, Sneddon A, Lopez V, Ellwood D. Impact of endometriosis on women's lives: a qualitative study. BMC women Health. 2014;14(123):1-12. [Link] [DOI:10.1186/1472-6874-14-123]
2. Dehvan F, Monjazebi F, Khanghahi ME, Mohammadi H, Gheshlagh R, Kurdi A. Adequacy of dialysis in Iranian patients undergoing hemodialysis: a systematic review and meta-analysis. Nephrol Urol Mon. 2018;10(5):e82235. [Link] [DOI:10.5812/numonthly.82235]
3. Prastiwi F, Wihastuti TA, Ismail DD. Factors associated with fatigue in chronic kidney disease patients undergoing hemodialysis: a systematic review. Jurnal Kedokteran Brawijaya. 2021;3(4):260-8. [Link] [DOI:10.21776/ub.jkb.2021.031.04.12]
4. Bagheban Karimi E, Lakdizaji S, Zamanzadeh V, Hasankhani H. The effects of infection control teaching on the knowledge and performance of hemodialysis nurses in Tabriz. Iran J Nurs. 2018;31(111). [Link] [DOI:10.29252/ijn.31.111.1]
5. Mottahedian TE, Najafi MS, Samiey S, Einllahi B, Babaei GH. Effect of programmed nursing care in prevention of hemodialysis complications. 2009;2(2):55-9. [Link]
6. Harris TJ, Nazir R, Khetpal P, Peterson RA, Chava P, Patel SS, et al. Pain, sleep disturbance and survival in hemodialysis patients. Nephrol Dial Transplant. 2012;27(2):758-65. [Link] [DOI:10.1093/ndt/gfr355]
7. Koirala N, Anvari E, McLennan G, editors. Monitoring and surveillance of hemodialysis access. Semin Intervent Radiol. 2016;33(1):25-30 [Link] [DOI:10.1055/s-0036-1572548]
8. Shechter SM, Skandari MR, Zalunardo N. Timing of arteriovenous fistula creation in patients with CKD: a decision analysis. Am J Kidney Dis. 2014;63(1):95-103. [Link] [DOI:10.1053/j.ajkd.2013.06.021]
9. Maghbool M, Khosravi T, Vojdani S, Chaijan MR, Esmaeili F, Amani A, et al. The effects of eugenol nanoemulsion on pain caused by arteriovenous fistula cannulation in hemodialysis patients: a randomized double-blinded controlled cross-over trial. Complementary therapies in medicine. 2020;52:102440. [Link] [DOI:10.1016/j.ctim.2020.102440]
10. Han B, Zhu FX, Shi C, Wu HL, Gu XH. Association between serum vitamin D levels and sleep disturbance in hemodialysis patients. Nutrients. 2017;9(2):139. [Link] [DOI:10.3390/nu9020139]
11. Asgari MR, Motlagh NH, Soleimani M, Ghorbani R. Effect of lidocaine spray on the pain intensity during insertion of vascular needles in hemodialysis patients. Koomesh. 2013;14(3):271-79. [Link]
12. Bayoumi MH, Mahmoud NF. Effect of education program on nurses' knowledge and practice regarding care of central venous line in pediatric hemodialysis: evidence-based practice guidelines. Egypt Nurs J. 2017;14(2):87-99. [Link] [DOI:10.4103/ENJ.ENJ_16_17]
13. Ghods A, Abfroosh N, Ghorbani R, Asgari M. Effect of lavender inhalation on pain intensity during insertion of vascular needles in hemodialysis patients. J Babol Univ Med Sci. 2014;16(10):7-14. [Link]
14. Nissenson AR, Fine RN, Mehrotra R, Zaritsky J. Handbook of Dialysis Therapy, E-Book: Elsevier Health Sciences; 2022. [Link]
15. Moosazadeh M, Nesami MB, Goudarzian AH. Effect of cryotherapy on arteriovenous fistula puncture-related pain in hemodialysis patients: a systematic review and meta-analysis. Complement Ther Med. 2020;49:102326. [Link] [DOI:10.1016/j.ctim.2020.102326]
16. Beladi Mousavi SS, Hayati F, Neseri I, Zeraati AA. Comparison of temporary dialysis catheter and AV fistula use at the time of starting chronic hemodialysis among end-stage renal diseases patients. J Mashhad Univ Med Sci. 2010;54(2):75-9. [Link]
17. Baloochi Beydokhti T, Ghadimifar A, Soleimani Moghaddam R. A comparative study on the effects of acupressure at SP6 and ST36 acupoints on the pain caused by fistula needle placement in hemodialysis patients. Complement Med J. 2021;10(4):354-67. [Link] [DOI:10.32598/cmja.10.4.975.1]
18. Ghani RMA. Effect of heat and cold therapy during the first stage of labor on women perception of birth experience: a randomized controlled trial. J Biol Agric Healthc. 2014;4(26):66-72. [Link]
19. Meissner W, Coluzzi F, Fletcher D, Huygen F, Morlion B, Neugebauer E, et al. Improving the management of post-operative acute pain: priorities for change. Curr Med Res Opin. 2015;31(11):2131-43. [Link] [DOI:10.1185/03007995.2015.1092122]
20. Arab V, Bagheri-Nesami M, Mousavinasab SN, Espahbodi F, Pouresmail Z. Comparison of the effects of Hugo point ice massage and 2% lidocaine gel on arteriovenous fistula puncture-related pain in hemodialysis patients: a randomized controlled trial. J Caring Sci. 2017;6(2):141. [Link] [DOI:10.15171/jcs.2017.014]
21. Modabber A, Rana M, Ghassemi A, Gerressen M, Gellrich NC, Hölzle F, et al. Three-dimensional evaluation of postoperative swelling in treatment of zygomatic bone fractures using two different cooling therapy methods: a randomized, observer-blind, prospective study. Trials. 2013;14:1-10. [Link] [DOI:10.1186/1745-6215-14-238]
22. Dryden T, Moyer CA. Massage therapy: Integrating research and practice: Human Kinetics; 2012. [Link] [DOI:10.5040/9781718210509]
23. Hausswirth C, Louis J, Bieuzen F, Pournot H, Fournier J, Filliard JR, et al. Effects of whole-body cryotherapy vs. far-infrared vs. passive modalities on recovery from exercise-induced muscle damage in highly-trained runners. PloS One. 2011;6(12):e27749. [Link] [DOI:10.1371/journal.pone.0027749]
24. Ichihashi S, Higashiura W, Itoh H, Sakaguchi S, Kichikawa K. Fracture and collapse of balloon-expandable stents in the bilateral common iliac arteries due to shiatsu massage. Cardiovasc Intervent Radiol. 2012;35:1500-4. [Link] [DOI:10.1007/s00270-011-0336-2]
25. Barani ZY, Shahraki M. Comparison of the effect of ice massage in the LI4 and SP6 on Primary Dysmenorrhea: a blinded clinical trial. Med Sci. 2018;22(94):544-8. [Link]
26. Kim M, Kim J. Effects of acupressure on pain, flexibility, and substance P in middle-age women with chronic neck pain. J Altern Complement Med. 2021;27(2):160-7. [Link] [DOI:10.1089/acm.2020.0413]
27. Hamidzadeh A, Shahpourian F, Orak RJ, Montazeri AS, Khosravi A. Effects of LI4 acupressure on labor pain in the first stage of labor. J Midwifery Womens Health. 2012;57(2):133-8. [Link] [DOI:10.1111/j.1542-2011.2011.00138.x]
28. Goddard G, Albers D. Effects of acupuncture at Large Intestine 4 (LI 4) on electrical tooth pulp stimulation: A randomized controlled pilot study. Med Acupunct. 2009;21(3):167-71. [Link] [DOI:10.1089/acu.2009.0691]
29. Khosravan S, Atayee P, Mazloum SSB, Mojtabavi SJ. Effect of Hugo's point massage with and without ice on vaccination-related pain in infants. J Hayat. 2018;24(21):7-19. [Link]
30. Al Amer HS, Dator WL, Abunab HY, Mari M. Cryotherapy intervention in relieving arteriovenous fistula cannulation-related pain among hemodialysis patients at the King Khalid Hospital, Tabuk, Kingdom of Saudi Arabia. Saudi J Kidney Dis Transpl. 2017;28(5):1050-6. [Link] [DOI:10.4103/1319-2442.215141]
31. Kaviani M, Ashoori M, Azima S, Rajaei Fard A, Hadian Fard M. Comparing the effect of two methods of acupressure and ice massage on the pain, anxiety levels and labor length in the point LI-4. JSSU. 2012;20(2):220-28. [Link]
32. Golda M, Revathi D, Subhashini N, Mathew J, Indira A. Assess the effectiveness of cold application on pre procedure (AV fistula puncture) pain among hemodialysis patients in tertiary care hospital, Nellore. Int J Appli Res. 2016;2(6):660-64. [Link]
33. Hosseinzadeh F, Alaee N, Rejeh N, Alemohammad S. Comparing the effect of cryotherapy and acupressure on pain intensity of arteriovenous fistula cannulation in patients hemodialysis. Iranian J Nurs Res. 2019;14(3):40-7. [Link]
34. Williamson A, Hoggart B. Pain: a review of three commonly used pain rating scales. J Clin Nurs. 2005;14(7):798-804. [Link] [DOI:10.1111/j.1365-2702.2005.01121.x]
35. Soltanpour F, Mohamadi N, Haghani H. Effect of huko point ice massage on pain degree during arterio venous fistula puncture in hemodialysis patients. Tehran: Tehran University of Medical Sciences;2012. [Link]
36. Porramezani N, Imani Goghary Z, Firouzabadi M, Balvardi M, Irannejad-Parizi F. The effect of cryotherapy in the Hoku point on the severity of pain of fistula catheterization in patients on hemodialysis. J Adv Med Biomed Res. 2019;27(124):37-42. [Link] [DOI:10.30699/jambs.27.124.37]
37. Davtalab E, Naji S, Shahidi S. Comparing the effects of valsalva maneuver and ice massage at Hoku point methods on pain intensity within the needle insertion to the arteriovenous fistula (AVF) for patients undergoing hemodialysis in the selected hospitals in Isfahan in 2015. Int J Med Res Health Sci. 2016;5(5):101-7. [Link]
38. Fareed AP, Abd El-Hay AH, El-Shikh AA. Cutaneous stimulation: Its effect on pain relieving among hemodialysis patients. J Educ Pract. 2014;5(1). [Link]
39. Page D, Taylor DM. Vapocoolant spray vs subcutaneous lidocaine injection for reducing the pain of intravenous cannulation: a randomized, controlled, clinical trial. Br J Anaesth. 2010;105(4):519-25. [Link] [DOI:10.1093/bja/aeq198]